🔑 Key Learning
- Common causes of vomiting, constipation, and obstruction in neonates and infants include pyloric stenosis, Hirschsprung’s, and duodenal atresia.
- Intussusception presents classically with episodic pain and redcurrant jelly stool.
- Toddler’s diarrhoea is benign and diagnosed clinically (peas and carrot stools)
- Always consider surgical referral for suspected obstruction or failure to pass meconium.
🥣 Infantile Hypertrophic Pyloric Stenosis
🧬 Pathophysiology
- Hypertrophy of the circular muscle of the pylorus causes gastric outlet obstruction.
👀 Clinical Features
- Age: 3–8 weeks
- Projectile, non-bilious vomiting within minutes of feeding
- Constipation, FTT
- Palpable ‘olive’ mass in RUQ
- Visible gastric peristalsis
🧪 Investigations
- 1st line: Abdominal USS: thickened pyloric muscle
- Biochemistry: Hypochloraemic, hypokalaemic metabolic alkalosis
💊 Management
- Ramstedt pyloromyotomy
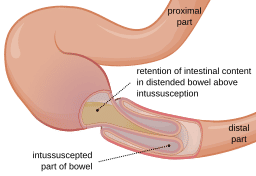
🎯 Intussusception
🧬 Pathophysiology
- Telescoping of proximal bowel into distal segment → obstruction, ischaemia
- Majority of cases occur in association with or following viral gastroenteritis/URTI
👀 Clinical Features
- Peak: 3–18 months
- Colicky episodic pain, drawing up legs
- Redcurrant jelly stool
- Palpable sausage-shaped mass (RUQ)
- Bilious vomiting, distension if progressed
🧪 Investigations
- USS: Target sign
- Contrast enema (diagnostic & therapeutic): Coiled spring appearance - gold standard.
💊 Management
- 1st Line: Therapeutic enema - air/water/contrast pumped into the colon, in an attempt to reduce the invagination, and restore the bowel to its normal position
- Surgery if unsuccessful or peritonitic
🌊 Duodenal Atresia
👀 Clinical Features
- Bilious vomiting within 48h of birth, begins following first oral feed
- Polyhydramnios antenatally
🧪 Investigations
- AXR: Double bubble sign
💊 Management
- Surgical: Duodenoduodenostomy
🥦 Toddler’s Diarrhoea (Chronic Non-Specific)
👀 Clinical Features
- A non-specific, chronic diarrhoea which most commonly affects children between 6 months and 5 years of age.
- Loose stools with undigested food (e.g. ‘peas and carrot stools’)
- Colicky pain, increased flatus
- Otherwise well and thriving with good development/growth.
💊 Management
- Reassurance
- Dietary: Reduce juice/milk, increase fat
- Loperamide rarely needed
🚫 Hirschsprung’s Disease
🧬 Pathophysiology
- Absence of ganglion cells in bowel (usually rectosigmoid) → functional obstruction
👀 Clinical Features
Neonates:
- Delayed meconium (>48 hrs), abdominal distension, bilious vomiting
- Older children:
- Chronic constipation since birth
- Poor response to laxatives
- FTT
🧪 Investigations
- AXR: Obstruction
- Rectal biopsy: Absence of ganglia

AXR in Hirschprung's. Public domain.
💊 Management
- Surgical resection of aganglionic segment
📝 Exam Clues & Clinchers
-
Pyloric stenosis: 3–8-week-old with projectile vomiting, palpable olive mass
- 1st line invx: Ultrasound
-
Intussusception: Intermittent colicky pain + redcurrant jelly stool
- Diagnostic/therapeutic enema
- Duodenal atresia: Bilious vomiting 24-48hrs after birth + double bubble sign on AXR
-
Hirschsprung’s: No meconium in first 48 hrs, chronic constipation
- Rectal biopsy!
- Toddler’s diarrhoea: Well child, undigested food in stool, resolves with age