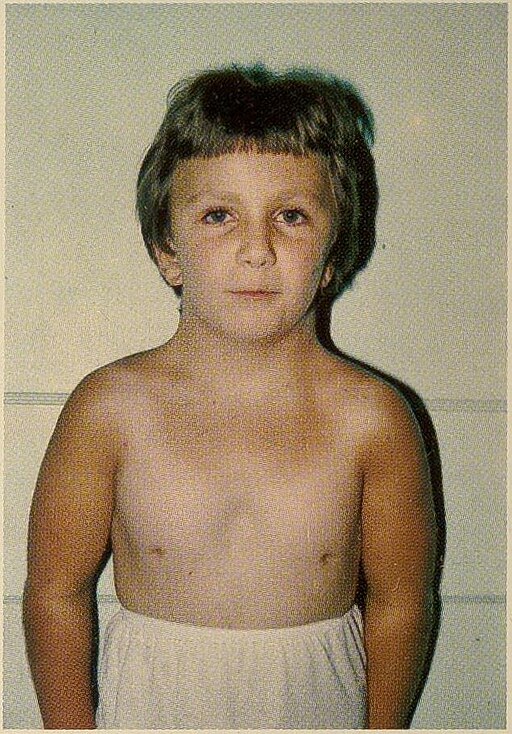
👶 Down Syndrome
Prevalence: 1/650 live births
Genetics: Trisomy 21 (95% due to nondisjunction during maternal oogenesis)
Clinical features:
- Generalised hypotonia and head lag at birth
- Facial features: up-slanting eyes, low-set ears, flat nasal bridge, epicanthic folds, protruding tongue, Brushfield spots (white specks in the iris)
- Short neck, brachycephaly (flat occiput)
- Single palmar crease, wide sandal gap between toes
- Learning disability, short stature
Complications:
- Congenital heart disease (50%) – AVSD most common
- Duodenal atresia
- Early-onset Alzheimer’s disease

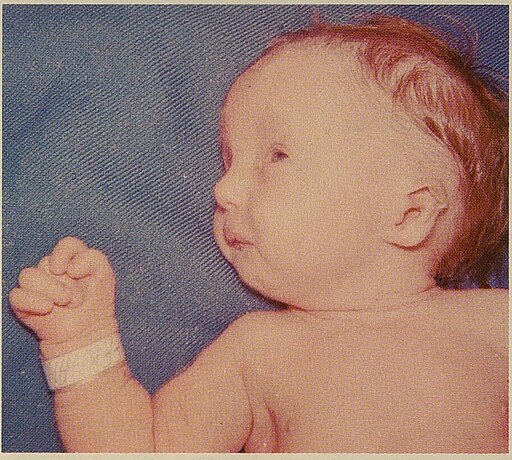
♀️ Turner Syndrome
Prevalence: 1/2500
Genetics: 45,X (monosomy X)
Clinical features:
- Female with short stature (growth falters after age 3–5)
- Webbed neck, low posterior hairline, widely spaced nipples (‘shield chest’)
- Neonatal lymphoedema – puffy hands and feet
- Cubitus valgus
- Primary amenorrhoea, infertility (streak ovaries)
Complications:
- Coarctation of the aorta
- Horseshoe kidney
Diagnosis: Karyotyping
😊 William’s Syndrome
Cause: Microdeletion on chromosome 7q11.23 (includes elastin gene)
Clinical features:
- Elfin facial appearance: full cheeks, wide mouth, full lips, periorbital fullness
- Overfriendly behaviour, anxiety, poor concentration
- Mild to moderate learning disability
- Hypercalcaemia in infancy (15%)
Complications: Supravalvular aortic stenosis
Diagnosis: FISH or chromosomal microarray

.
🧠 Patau Syndrome
Prevalence: 1/4000
Genetics: Trisomy 13 (usually maternal nondisjunction)
Clinical features:
- Small for gestational age
- Microcephaly, holoprosencephaly
- Cleft lip and palate, microphthalmia
- Polydactyly
- Fused kidneys
Prognosis: Very poor – most die within days to weeks
Diagnosis: Antenatal US and confirmed by karyotype

🧠 Edward’s Syndrome
Prevalence: 1/6000
Genetics: Trisomy 18
Clinical features:
- Females > males
- Small size, micrognathia
- Overlapping fingers, clenched hands
- Rocker-bottom feet
Prognosis: Very poor – median lifespan 4 days
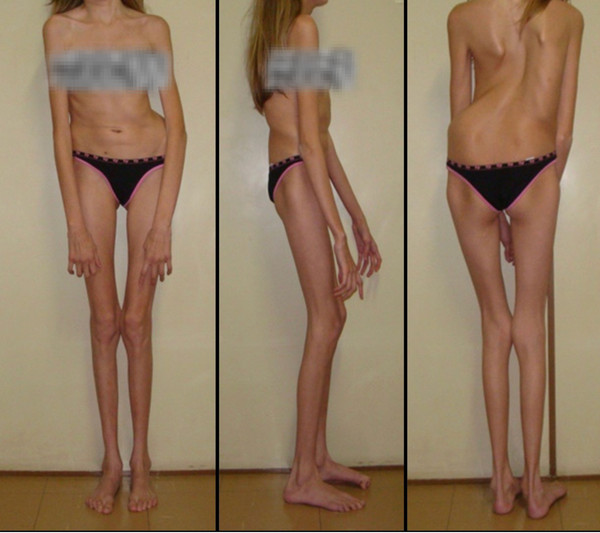
🍽 Prader-Willi Syndrome
Prevalence: 1/10,000
Genetics: Deletion on paternal chromosome 15 (15q11-q13)
Clinical features:
- Neonatal hypotonia, poor feeding, failure to thrive
- Rapid weight gain from 1 year
- Truncal obesity, short stature
- Food foraging, insatiable appetite
- Mild learning difficulties
♂️ Klinefelter Syndrome
Prevalence: 1/500 males
Genetics: 47,XXY (nondisjunction)
Clinical features:
- Tall stature, reduced facial/body hair
- Pubertal testicular involution – small, firm testes
- Gynaecomastia
- Infertility (azoospermia)
- Mild learning difficulties
Diagnosis: Karyotype
Endocrine profile: Hypergonadotrophic hypogonadism – high LH/FSH, low testosterone
.
🕷 Marfan Syndrome
Prevalence: 1/5000
Genetics: Autosomal dominant – FBN1 gene mutation (chr15q21)
Clinical features:
- Tall, slim, long limbs – arachnodactyly
- High arched palate, scoliosis, joint hypermobility
- Positive wrist/thumb signs
- Pectus excavatum or carinatum
- Mitral valve prolapse (mid-systolic click), aortic root dilatation – risk of dissection
Management: Regular echo, beta-blockers or ARBs, avoid contact sport
👨⚕️ Noonan Syndrome
Prevalence: 1/2500
Genetics: Autosomal dominant – PTPN11 mutation (chr12)
Clinical features:
- Webbed neck, short stature, hypertelorism
- Chest deformity (pectus carinatum/excavatum)
- Undescended testes
- Mild learning difficulty
- Congenital heart defects – pulmonary stenosis most common
👃 DiGeorge Syndrome
Prevalence: 1/4000
Genetics: Microdeletion on chromosome 22q11.2
Clinical features:
- Subtle facial dysmorphism – small mouth, bulbous nasal tip
- Cleft palate, speech delay
- Hypocalcaemia (parathyroid hypoplasia)
- Immunodeficiency (thymic aplasia)
- Congenital heart disease – TOF, interrupted aortic arch
🧫 Phenylketonuria (PKU)
Genetics: Autosomal recessive, PAH gene mutation (chromosome 12)
Pathophysiology:
- Deficient phenylalanine hydroxylase → toxic phenylalanine accumulation
- Interferes with brain neurotransmitter synthesis
Clinical features:
- Detected on newborn heel prick screening
- If untreated: intellectual disability, seizures, eczema, musty body odour, pale skin/hair
Management:
- Low phenylalanine diet, tyrosine supplementation
🧩 Neurofibromatosis
Genetics: Autosomal dominant
NF1
Gene: NF1 (chromosome 17)
Diagnosis: ≥2 of:
- ≥6 café-au-lait spots
- Axillary or inguinal freckling
- ≥1 neurofibroma or plexiform neurofibroma
- Optic glioma
- ≥1 Lisch nodule (iris hamartoma)
- Bony dysplasia
- 1st-degree relative with NF1
NF2
Gene: NF2 (chromosome 22)
Features:
- Bilateral vestibular schwannomas (hallmark)
- Meningiomas, ependymomas, cataracts
- Sensorineural deafness or balance problems

🧠 Tuberous Sclerosis Complex (TSC)
Genetics: Autosomal dominant – mutations in TSC1 (hamartin) or TSC2 (tuberin)
Clinical features:
- Skin: Facial angiofibromas, ash-leaf patches, shagreen patches, periungual fibromas
- CNS: Seizures, developmental delay, subependymal nodules or giant cell astrocytomas
- Kidneys: Renal angiomyolipomas – haematuria or rupture
- Heart: Rhabdomyomas
- Eyes: Retinal hamartomas
- Behavioural: Autism, ADHD

.
📝 Exam Clues & Clinchers
- Down syndrome: hypotonia, single palmar crease, AVSD
- Turner: short female with primary amenorrhoea, webbed neck, coarctation
- William’s: elfin face, hypercalcaemia, friendly personality, supravalvular AS
- Patau: microphthalmia, cleft lip, polydactyly, holoprosencephaly
- Edward’s: rocker-bottom feet, overlapping fingers, small jaw
- Prader-Willi: hyperphagia, truncal obesity, short stature
- Klinefelter: tall male, small testes, gynaecomastia, XXY
- Marfan: tall, lens dislocation, aortic root dilatation
- DiGeorge: cleft palate, hypocalcaemia, congenital heart disease
- PKU: fair hair/skin, intellectual disability, musty odour
- NF1: café-au-lait, axillary freckling, Lisch nodules
- NF2: bilateral acoustic neuromas
- TSC: seizures + skin findings (ash-leaf, shagreen)