Also known as pruritic urticarial papules and plaques of pregnancy (PUPPP)
Intensely itchy, third trimester rash
Starts in abdominal striae as pink papules → urticarial plaques
May spread to trunk and limbs
Resolves after delivery
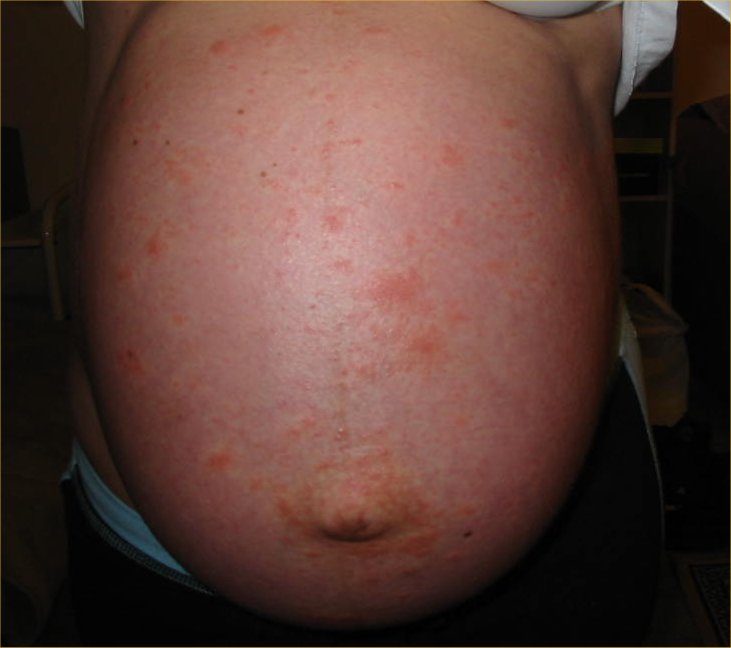
Left side view of the abdomen at nearly 36 weeks' gestation, showing the papules and plaques of PUPPP.Frontal view of the abdomen at nearly 36 weeks' gestation, on which the papules and plaques of PUPPP can clearly be seen
Management
Antihistamines
Topical corticosteroids (oral if severe)
Pemphigoid Gestationis
Pathophysiology
An autoimmune, blistering rash of pregnancy
An IgG autoantibody (called PG factor) develops and targets BP-180 proteins within the basement membrane between the epidermis and dermis.
Clinical Features
Starts around umbilicus in second or third trimester
Urticarial rash → tense fluid-filled blisters
May spread to trunk, limbs, buttocks
Management
Topical corticosteroids if mild
Systemic corticosteroids if severe
📝 Exam Clues & Clinchers
Pregnancy + leg swelling → suspect DVT → duplex US
Suspected PE + DVT symptoms → US first; if positive, no need to do CTPA
Hyperthyroid in pregnancy → PTU in first trimester, switch to carbimazole later
Itchy palms/soles + raised bile acids in late pregnancy → obstetric cholestasis
ALT > 500 + third trimester + acute hepatitis signs → acute fatty liver