🍇 Gestational Trophoblastic Disease
🔑 Key Learning
-
GTD includes molar pregnancy, choriocarcinoma, invasive mole, and placental site trophoblastic tumour.
-
Presents in early pregnancy with abnormal PV bleeding, hyperemesis, and markedly raised β-hCG.
-
Ultrasound shows a classic "snowstorm” or "bunch of grapes" appearance.
-
Managed with uterine evacuation and serial β-hCG monitoring to detect persistent disease.
🧬 Pathophysiology
-
Abnormal trophoblastic proliferation due to atypical fertilisation events.
- The spectrum of GTD includes:
-
Complete mole
-
Partial mole
-
Choriocarcinoma
- Placental site trophoblastic tumour
👀 Clinical Features
-
Abnormal vaginal bleeding in 1st trimester (6–12 weeks) - spotting to heavy bleeding
-
Uterus larger than expected for gestational age
-
Severe hyperemesis gravidarum
-
Early-onset pre-eclampsia (rare, severe cases)
-
Symptoms of hyperthyroidism (due to β-hCG cross-reactivity with TSH receptor)
🧪 Investigations
-
Transvaginal ultrasound:
-
“Snowstorm” or “bunch of grapes” appearance
-
No identifiable foetus in complete mole
-
Serum β-hCG:
-
Markedly raised, much higher than expected for gestational age
-
Histology:
-
Hydropic villi, trophoblastic hyperplasia (diagnostic post-evacuation)
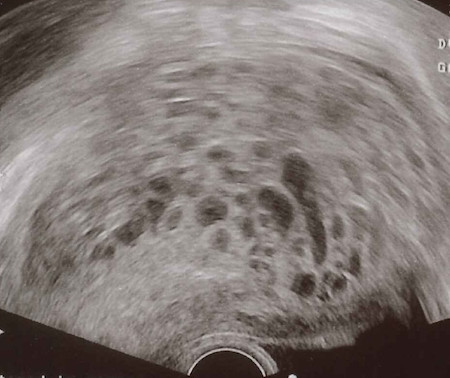 Figure 203: US molar pregnancy: A "snowstorm" or "bunch of grapes" appearance, due to multiple cystic structures.
Figure 203: US molar pregnancy: A "snowstorm" or "bunch of grapes" appearance, due to multiple cystic structures.
💊 Management
-
Uterine evacuation by suction curettage under general anaesthetic
-
Serial serum β-hCG monitoring until normal for 6 consecutive months
-
Contraception advised during follow-up (avoid pregnancy while β-hCG is monitored)
-
Chemotherapy (e.g. methotrexate) if:
-
β-hCG plateau or rise
-
Histology confirms invasive mole or choriocarcinoma
-
Placental site trophoblastic tumour often requires surgical resection
📝 Exam Clues & Clinchers
-
1st trimester bleeding + uterus large for dates + hyperemesis + very high β-hCG
-
Snowstorm appearance on ultrasound

